Vitamin D is one of the most essential nutrients for human health. It plays a role in bone development, calcium absorption, immune function, and even mood regulation. Unlike most vitamins, however, Vitamin D isn’t primarily obtained from food — it is made in the skin when ultraviolet B (UVB) rays from the sun trigger a chemical reaction involving 7-dehydrocholesterol in human skin. This unique requirement makes sunlight not just helpful, but central to human biology.
In theory, sunlight should make Vitamin D deficiency rare. After all, billions of people around the world live in sunny regions where UVB light is abundant year-round. Yet paradoxically, Vitamin D deficiency is widespread — even in places where sunshine is plentiful. Research shows that South Asia, Southeast Asia, and the Middle East have particularly high rates of deficiency despite strong sunlight through much of the year. This disconnect between nature’s design and health outcomes speaks not only to biology, but to how we live.
Sunlight: Nature’s Vitamin D Factory
To understand why deficiency exists at all, it helps to review how Vitamin D synthesis works. When UVB radiation hits the skin, it converts a precursor molecule into previtamin D3, which then becomes Vitamin D3 and enters the bloodstream. Without enough UVB exposure, this process falters, lowering serum levels of Vitamin D.
Doctors and scientists use serum 25-hydroxyvitamin D [25(OH)D] levels as the main measure of Vitamin D status. Levels below certain thresholds are associated with diseases such as rickets in children — skeletal deformities caused by insufficient calcium absorption — and osteomalacia in adults. Low Vitamin D has also been linked to compromised immunity, muscle weakness, and even increased risk for certain chronic diseases.
Yet even in regions with abundant sun, studies show startling levels of deficiency. In South Asia, for example, estimates suggest more than 65–70 % of adults are deficient. A systematic review among pregnant women in South Asia found a pooled prevalence of 65 % insufficiency — a level high enough to warrant public health attention. These figures are hardly isolated; globally, nearly three quarters of people have serum Vitamin D levels below what is considered sufficient.
The Paradox of Plenty
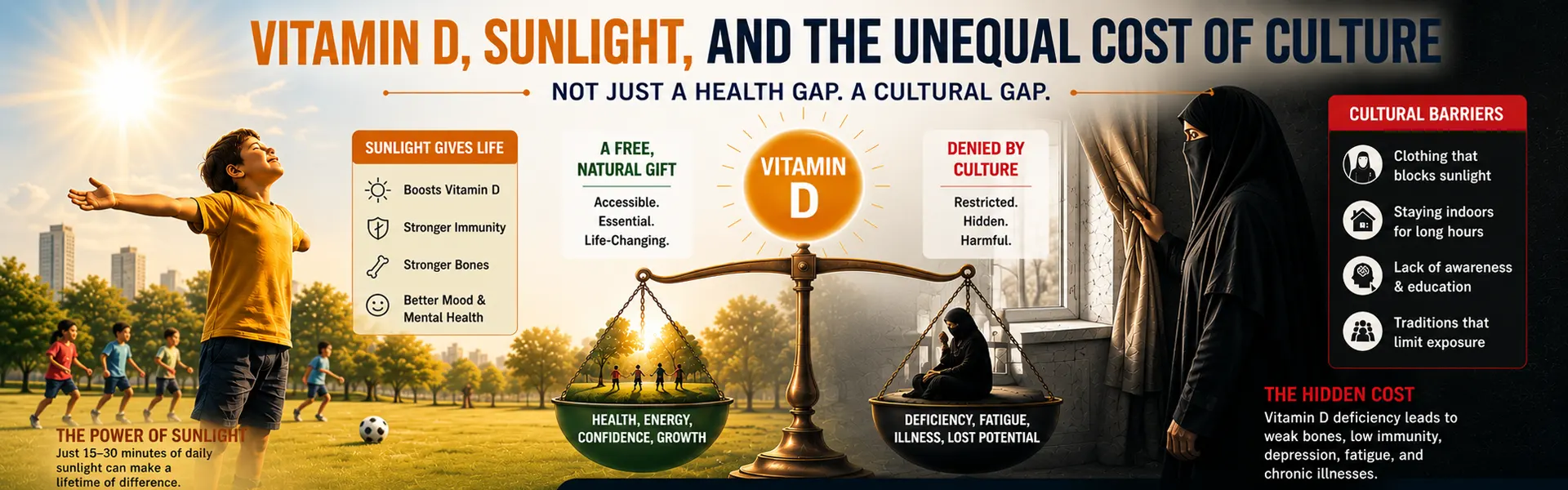
Why does deficiency persist where sunlight is abundant? Part of the answer is lifestyle, environment, and behavior. Urban living, air pollution, indoor jobs, sunscreen use, and even skin pigmentation affect how much UVB actually reaches the skin. But another significant factor — one that is less discussed in public health conversations — is how culture and social norms influence sun exposure.
In many societies, particularly conservative ones, social norms surrounding modesty and dress effectively limit skin exposure to sunlight, especially for women. While the intent may be rooted in cultural or religious values, the biological consequence is clear: less exposed skin means dramatically less opportunity for the UVB that drives Vitamin D production. Studies have documented that clothing styles that cover most of the skin reduce the amount of sunlight that reaches it, increasing the risk of deficiency.
A national study in Saudi Arabia, for example, found that more than 70 % of young women have Vitamin D deficiency, and one of the main contributing factors was limited sun exposure linked to traditional dress and indoor lifestyles. Research across Asia and the Middle East similarly ties cultural behaviors and life patterns to lower Vitamin D levels — despite the intensive sunlight these regions receive.
These findings reveal a sobering contrast. Nature has made sunlight available to nearly everyone, yet social norms can obstruct access to it. In effect, the biology of health collides with human culture, and in this collision, some groups — especially women — end up bearing the cost.
Unequal Biology in an Unequal World
Some may argue that limited sun exposure is simply part of cultural practice — a moral choice, a sign of modesty, or a designated lifestyle. But framing the issue as a moral one ignores the biological facts. If Vitamin D production depended on something other than sunlight — say, light filtering through clothing or indoor environments — then deficiency would be unlikely even when skin is fully covered. But that is not how physiology works.
In fact, Vitamin D synthesis is uniquely dependent on direct UVB exposure to unshaded skin. No amount of traditional clothing can trigger the same biochemical reactions. This isn’t a moral judgment about dress; it is a statement about human biology.
When societies treat sun avoidance or full covering as preferable to direct exposure without acknowledging the health trade-offs, they create an environment where deficiency becomes normalized. Doctors see it; researchers report it; individuals experience fatigue, muscle weakness, and compromised immunity. Yet the silent acceptance of limited sun exposure becomes woven into the cultural fabric, sometimes explained away with references to fate or divine will rather than structural patterns of living.
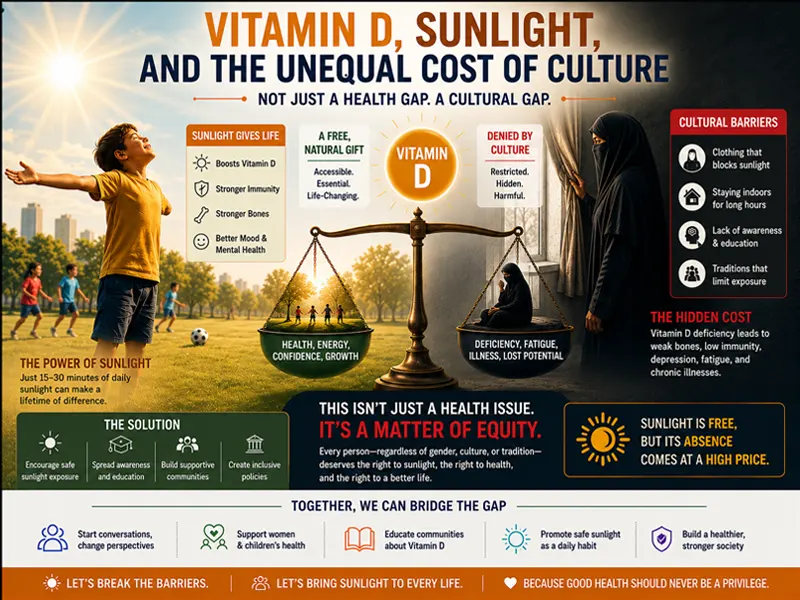
Vitamin D’s relationship with sunlight is a fact of human biology — not a moral judgement, not a theological statement, but a biochemical reality encoded in our skin. When social norms limit access to sunlight, they are not making us morally superior — they are creating conditions that make deficiency more likely, particularly among women and other vulnerable groups.
It’s time for a balanced conversation that recognizes both cultural values and biological needs. Health should not be an afterthought in cultural practice. When belief systems and biology conflict, the body pays the price first. Understanding that price is the first step toward changing the narrative — from one of passive acceptance to one of informed, empowered choice.